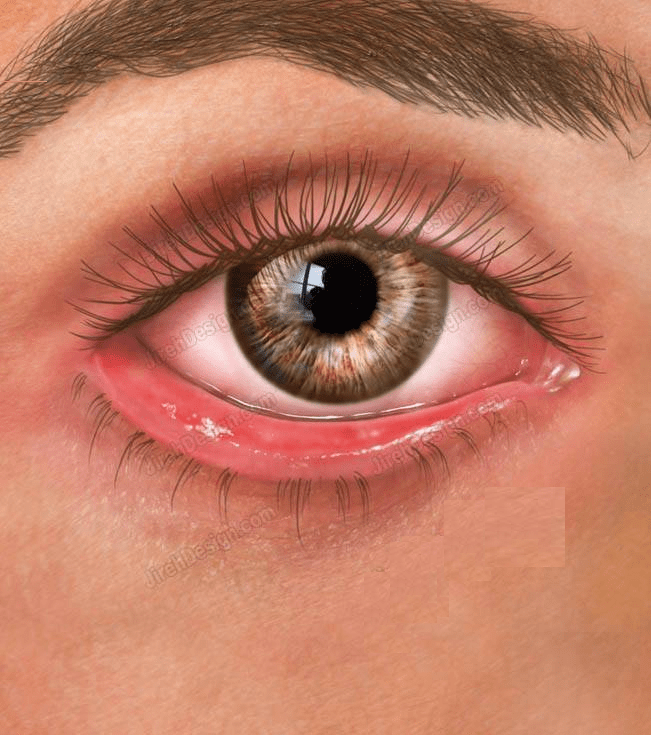
Ectropion
lecture Dr. Fawaz al Sarayeh
Eversion of the led to the out side. Causes of ectropion are:
■ Age-related.
■ Cicatricial: due to shortage of skin – may occur with ageing, trauma, previous lower lid surgery, chronic over flow of tears/topical medication.
■ Paralytic: e.g. facial nerve palsy due to any cause.
■ Mechanical: from a lower lid mass such as a meibomian cyst or neoplasia.
Symptoms
Epiphora ( teary eyes) , intermittent red eye, mucous discharge.
Signs
Part or whole of the lower lid is everted from the globe. Other changes may be present, e.g. dermatochalasis, ptosis, punctal stenosis.
What to ask and what to examine in those patients :
firstly assess and ask for history of trauma, and facial nerve power.
1. Age-related:
■ Horizontal laxity: lower lid fails to snap back when distracted from the globe.
■ Lateral and medial canthal ligament laxity: note the degree of punctal displacement with’ lateral traction, e.g. to the medial limbus or medial pupil.’
■ Retractor laxity causing tarsal (shelf) ectropion: the tarsal conjunctiva may be infl amed/thickened from chronic exposure; punctal stenosis is commonly present.
■ Orbicularis muscle hypotony: assess for lagophthalmos, upper lid retraction, assess Bell’s phenomenon, upgaze, and corneal sensation.
2. Anterior lamella cicatricial changes:
■ Ask the patient to open his/her mouth and look up. In the presence of significant cicatricial changes, the lid cannot be apposed to the globe.
■ Assess the extent of available skin in the upper lids and pre/postauricular areas as part of surgical planning.
Investigations A lower lid mass causing ectropion may require biopsy and appropriate excision.
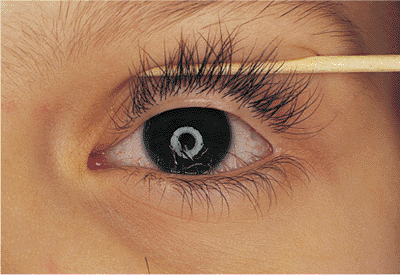
Floppy Eyelid Syndrome
Typically presents in middle-aged obese men with unilateral or bilateral chronic papillary conjunctivitis, marked upper lid tissue laxity, and spontaneous tarsal eversion at night.
Frequently associated with sleep apnoea syndrome. The aetiology is unknown but histology shows decreased elastin in the tarsus.
Symptoms Irritable red eye. Upper lid eversion at night (on the sleeping side).
Signs Easily everted tarsus (Fig. 1.7) with rubbery consistency, lash ptosis, papillary conjunctivitis, and superior punctate keratitis.
History and examination The patient’s partner may report heavy snoring, apnoea and lid eversion at night. Horizontal lid laxity is usually marked. Keratitis may be subtle.
Entropion:
inward eversion of the lid.
Classification
■ Congenital.
■ Acquired: age-related, cicatricial, mechanical
Symptoms Epiphora, mucous discharge and red eye.
Signs All or part of the lower lid may be inverted. Other features include: subtarsal mucous strands, lash–cornea touch, punctate epithelial keratopathy, conjunctival cicatricial changes, punctal stenosis, skin laxity, preseptal orbicularis riding upwards (‘spastic entropion’).
History and examination Ask about previous lid surgery and cicatrizing disease, e.g. Steven-Johnson’s syndrome, ocular mucous membrane pemphigoid (OMMP) and allergy to topical medication. Forced lid closure may elicit subtle entropion. Exclude effacement of the plica, an early sign in OMMP. Lower lid entropion may simulate distichiasis. In the former, the meibomian gland orifices are always found posterior to the lashes.
Investigations Conjunctival biopsy if OMMP suspected.
———————————————————————————-
Trichiasis : Eyelash follicles are in a normal position (unlike distichiasis) but directed towards the globe . Causes include chronic lid margin disease (Blepharitis) and conjunctival cicatricial diseases, e.g. Stevens-Johnson syndrome and ocular mucous membrane pemphigoid.
Treat small numbers of lashes with electrolysis, but up to half may re-grow, and treatment may cause tarsal scarring and further trichiasis. Full-thickness lid excision with repair of the defect is a more permanent treatment for localized trichiasis. Manage more extensive areas with cryotherapy. but be aware that this may cause localized skin depigmentation in dark skinned patients; electrolysis and correction of any lid margin malposition may be preferable in such patients.
——————————————————————————————
Distichiasis
Clinical features
In contrast to trichiasis, distichiasis is a congenital disorder in which a separate and more posterior row of metaplastic lashes exists (often growing out of the meibomian gland orifices). The lid margin is in a normal position
Management
■ If only a few lashes are affected, evert the eyelid with a meibomian clamp, use a microscope and incise the shaft of the eyelash through the partial thickness of the tarsus to the hair bulb. Electrolyse it under direct vision.
■ More extensive areas can be treated by splitting the lid at the grey line, freezing the posterior lamella, and suturing the lamella back together. The posterior lamella must be advanced to compensate for the shrinkage after cryotherapy, which could lead to subsequent entropion formation.
