
There are no pathognomonic features of neoplasia, but a careful history may identify a gradually enlarging lid lesion, crusting, bleeding, irritation, red eye, and epiphora due to mechanical ectropion, corneal irritation, or involvement of the lacrimal drainage system. A biopsy is indicated to exclude malignancy.
Premalignant disease
■ Actinic keratosis: 20% of cases may progress to squamous cell carcinoma. Lesions may be widespread and a dermatology opinion may be required. Treat by excision or cryotherapy.

■ Bowen’s disease (intraepithelial neoplasia): cellular atypia is present at the level of the basement membrane, but no deeper. Progresses to squamous cell carcinoma in 2–3% of
cases; most advocate complete excision unless there is limited tissue, such as around the canaliculi. Such cases are managed by debulking and cryotherapy, with full excision
in cases of malignant transformation.

■ Lentigo maligna: slowly spreading macular lesion, with irregular border. Become infiltrative in 33% of cases. Complete excision is preferable, but where this is impractical,
the area needs to be monitored closely, with excisional biopsy, performed on any enlarging or suspicious areas

Primary eyelid malignant disease
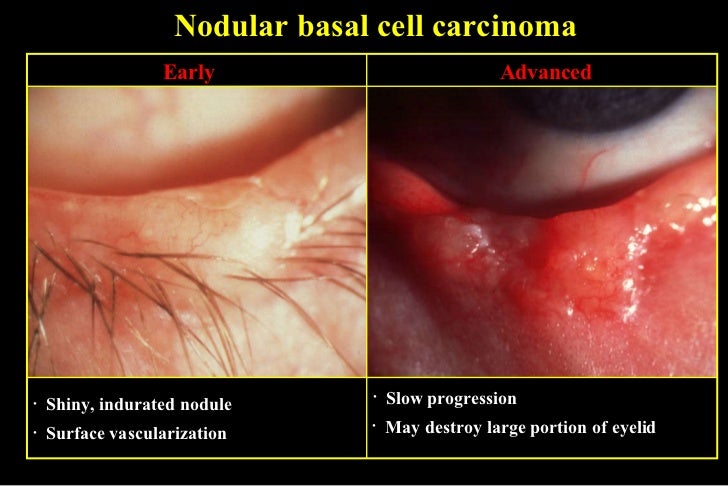
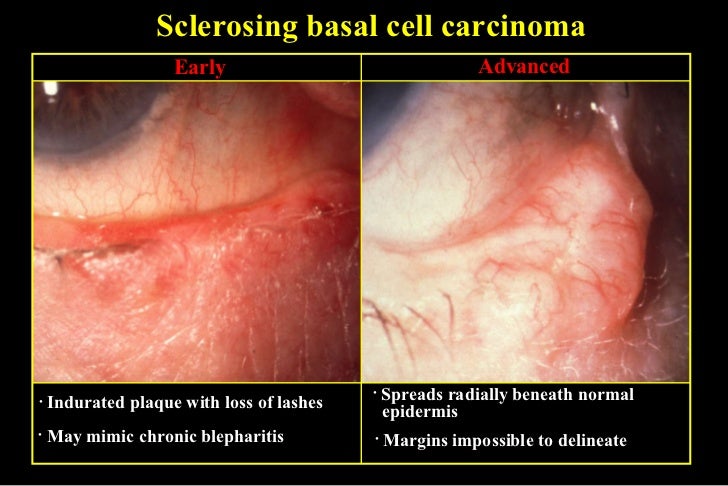
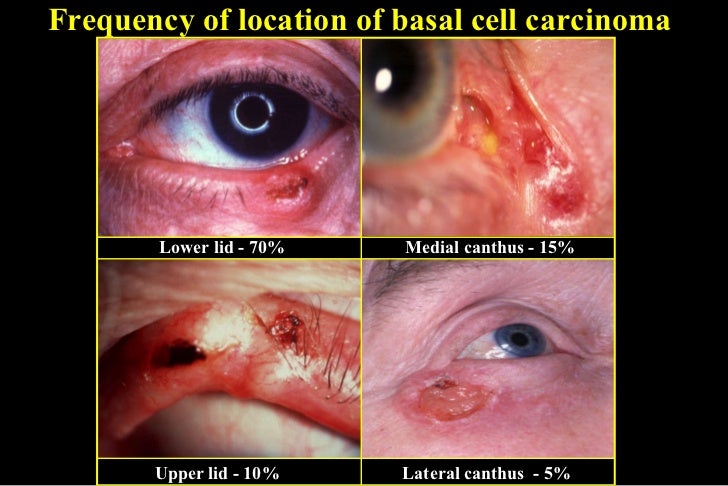
- Basal cell carcinoma BCC accounts for >90% of all neoplastic eyelid lesions, being most prevalent in fair-skinned individuals. Subtypes are described as nodular, ulcerative, cystic, sclerosing, pigmented or morphoeiform, the latter being the most difficult to manage. Lesions occur most commonly on the lower lid and medial canthus, and may be raised (nodular) or flat (e.g. morphoeiform). Other features include destruction of the lash follicles, a raised pearly edge with telangiectatic vessels, ulcerated centre, cyst formation, and pigmentation.

Complete excision with minimal sacrifice of healthy tissue is achieved by Mohs’ micrographic surgery, where available. Margin control may also be achieved with frozen section or fast paraffin. Close communication with the histologist is essential. Reconstruction may entail direct closure for small margin tumours, local sliding myocutaneous flaps, and/or full thickness skin grafting for anterior lamella defects. Posterior lamella defects may be reconstructed with local conjunctival advancement, free tarsoconjunctival graft from the upper lid, hard palate graft, and nasal mucosal or labial mucosal grafts. Very small eyelid lesions, and those in elderly, frail patients, may be managed with cryotherapy. Local radiotherapy is not useful; subsequent lesion recurrence may be as high as 20% and may be difficult to control. Chemotherapy plays no role. Distant metastases are exceptionally rare.
- Squamous cell carcinoma; SCC represent ≈5 % of all eyelid malignancies. Lesions occasionally develop from preexisting areas of actinic keratosis or Bowen’s disease. Typically present as a thickened, erythematous scaly lesion, but may also resemble BCC. Surface keratinization may be marked. SCC is more aggressive than BCC, with ≈5% of patients developing local periocular recurrence despite histologically complete excision. Excision and reconstruction principles are similar to BCC. SCC has a metastatic potential; mortality is due to local perineural spread to the CNS (≈2 %). The alternative to surgical excision includes cryotherapy which is good for small lesions, particularly those close to the lacrimal drainage apparatus. Radiotherapy is effective but is preferably avoided on the upper lid, because of the risk of inducing an irritable eye from keratin production on the tarsal conjunctiva, and for lesions at the medial canthus, which may extend deeply.

- Sebaceous gland carcinoma: A rare, aggressive tumour which commonly arises from the meibomian glands. It carries a high morbidity due to local, haematogenous, and lymphatic spread. A history of presumed recurrent chalazion
or a chronic unilateral blepharoconjunctivitis should raise suspicion.

Early diagnosis and complete excision is essential. Mapping biopsies of the superior and inferior tarsal and bulbar conjunctiva are performed to exclude multicentric origin and pagetoid spread. The histologist should be alerted to use the appropriate lipid stains. Orbital exenteration is indicated in patients with diffuse involvement of the lid or conjunctiva. Radiation therapy plays a palliative role. - Melanoma: represents <1 % of eyelid neoplasms. Lesions are irregularly pigmented, but a large minority may lack pigmentation. Other features include infl ammation and bleeding. Clinical forms include lentigo maligna, superficial spreading, and nodular melanoma. Metastases are common in the latter two forms. The Breslow thickness predicts the average time to metastasis. The cure rate for lesions
<0.75 mm thick approaches 100%.
Excise lesions <1.5 mm thick with wide margins and reconstruct. Lesions >1.5 mm require additional neck lymph node scintigraphy and biopsy. Involve nuclear medicine, and head and neck or plastic surgery colleagues. Distant metastasis may occur even with clear histological margins.

