
Dr. Fawaz al sarayreh lecture
PPT Dr. Fawaz lecture
Written By Khalil AL-Salem M.D
Anatomy and physiology :
Diabetic Retinopathy
Diabetics can lose vision from macular oedema, macular ischaemia, vitreous haemorrhage, and tractional retinal detachment. The ophthalmologist has several tasks: 1- confirm the diagnosis;
2- classify its severity and monitor accordingly;
3- offer advice; apply retinal laser as required;
4- treat associated eye disease such as cataract.
Key studies (للعلم و الإستزادة ، غيرمطلوب من سنه خامسة )
■ Diabetic Retinopathy Study (DRS): defined high-risk proliferative diabetic retinopathy and risk of severe visual loss with different levels of retinopathy.
Established that panretinal photocoagulation (PRP) decreases the risk of severe visual loss in high-risk PDR.
■ Wisconsin Epidemiologic Study of Diabetic Retinopathy (WESDR): population-based study showed that glycosylated haemoglobin levels and duration of diabetes are risk factors for progression of retinopathy.
■ Early Treatment of Diabetic Retinopathy Study (ETDRS): defined clinically significant macular oedema and showed that laser treatment approximately halves the risk of
moderate visual loss.
■ Diabetic Retinopathy Vitrectomy Study (DRVS): demonstrated that early vitrectomy for vitreous haemorrhage (within 3 months) improved visual prognosis in type 1 diabetes.
■ Diabetes Control and Complications Trial (DCCT): demonstrated that intensive insulin treatment reduced the risk of sustained progression of retinopathy in type 1 diabetes when compared to conventional insulin treatment.
■ United Kingdom Prospective Diabetes Study (UKPDS): showed that tight blood pressure and glycaemic control in type 2 diabetes reduced retinopathy progression and visual loss.
Classification of diabetic retinopathy (مهم جدا و مطلوب)
■ Mild non-proliferative diabetic retinopathy (NPDR): At least one microaneurysm.
■ Moderate non-proliferative diabetic retinopathy: intraretinal haemorrhages or microaneurysms < ETDRS standard photograph 2a (Figure bellow) and/or cotton-wool spots, venous beading, intraretinal microvascular abnormalities (IRMA).
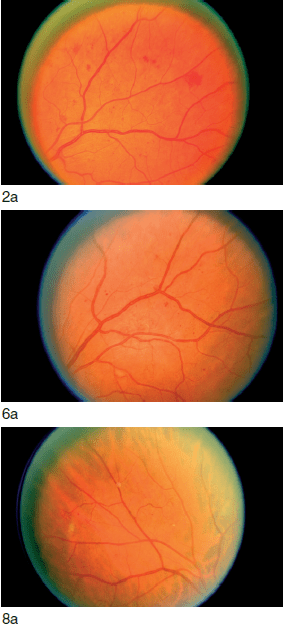
(Courtesy ETDRS Research Group.)
■ Severe nonproliferative diabetic retinopathy: relies on the 4–2-1 rule, which requires one of the following:
1. Intraretinal haemorrhages or microaneurysms in four quadrants.
2. Venous beading ≥ ETDRS photograph 6a in
two quadrants.
3. IRMA ≥ ETDRS photograph 8a in one
quadrant.
■ Very severe non-proliferative diabetic retinopathy: at least two of the criteria for severe NPDR.
■ Non-high risk proliferative diabetic retinopathy: new vessels on the disc (NVD) or elsewhere (NVE), but criteria not met for
high-risk proliferative diabetic retinopathy (PDR) below.
■ High-risk proliferative diabetic retinopathy: at least one of the following:
1. NVD >1/3 disc area.
2. NVD plus vitreous or preretinal haemorrhage.
3. NVE >1/2 disc area plus preretinal or vitreous haemorrhage.
■ Advanced proliferative diabetic retinopathy: tractional retinal detachment.
Macular exudates or thickening can occur with any severity of retinopathy.
Treatment is advised if there is clinically significant macular oedema (CSMO) comprising at least one of the following:
■ Thickening of the retina within 500 μm of the fovea.
■ Hard exudates located within 500 μm of the fovea with adjacent retinal thickening.
■ Retinal thickening at least one disc area in size, part of which is located within one disc diameter of the fovea.
History Ask about the duration and type of diabetes, blood sugar control, smoking and associated disease, especially hypertension and renal disease. Identify the clinicians monitoring the patient’s diabetes.
Examination Examine the iris at high magnification for neovascularization (NVI). If present, or if IOP is elevated, perform gonioscopy to look for angle neovascularization (NVA). Perform careful fundus examination looking for atypical features. Exclude
associated disease, especially posterior subcapsular cataracts.
Classify severity.
Differential diagnosis
■ Nonproliferative diabetic retinopathy: central or branch retinal vein occlusion; ocular ischaemic syndrome; hypertensive retinopathy; radiation retinopathy; leukaemia; anaemia; HIV microangiopathy.
■ Proliferative diabetic retinopathy: vascular obstruction; sickle cell retinopathy; ocular ischaemic syndrome; sarcoidosis; Eales’ disease; tuberculosis; embolization from intravenous drug use.
Investigations Check blood pressure and fasting glucose if not diagnosed diabetic. Arrange fluorescein angiography if CSMO is present (to guide laser treatment) or if there is unexplained poor vision (to assess macular ischaemia).
Ocular management depends on the findings:
■ Nonproliferative diabetic retinopathy.
1. Absent or mild: refer to screening program for annual review (1% risk of high-risk PDR in 1 year).
2. Moderate: review 6–9 monthly (4% risk of high-risk PDR in 1 year).
3. Severe: review 4–6 monthly (8% risk of high-risk PDR in 1 year).
4. Very severe: review 3–4 monthly (17% risk of high-risk PDR in 1 year).
■ Proliferative retinopathy.
1. Non-high risk: review in 2 months (50% risk of high-risk PDR in 1 year). Consider PRP if poor attendance or poor diabetic control.
2. High-risk or iris new vessels: perform PRP within 1 week, preferably immediately. If there is coexisting CSMO, perform macular laser treatment first or at the same time.
■ Vitreous haemorrhage.
Treat mild vitreous haemorrhage as high-risk PDR. If the haemorrhage is dense enough to obscure the fundal view, perform B-scan ultrasound to exclude retinal detachment.
Review monthly to monitor for iris new vessels or raised IOP. Apply PRP as haemorrhage clears and the view improves. Arrange vitreoretinal review if the haemorrhage persists for 1 month (type 1 diabetes), or 3–4 months (type 2). Consider early referral if the other eye has poor accuity.
■ Tractional retinal detachment.
If tractional retinal detachment threatens the macula, arrange vitreoretinal review. If not, review 2–3 monthly depending on the retinopathy severity.
■ Maculopathy.
1. Not clinically significant: review in 4–6 months.
2. Clinically significant macular oedema: perform fluorescein angiography unless there is an isolated circinate, and treat as per ETDRS:
a. Focal laser to circinate ring.
b. Modified grid to areas of macular thickening.
c. Macular grid for diffuse thickening.
d. Avoid laser treatment to the edge of, or within, the foveal avascular zone (FAZ).
Consider earlier review for all categories if there is poor diabetic or blood pressure control, or recent marked improvement in diabetic control (can transiently worsen retinopathy).
Examples of Diabetic retinopathy :


