
Preoperative Assessment
Cataract is the most common cause of treatable blindness worldwide. Most cataracts are age-related. An estimated 30% of those aged over 65 have visually significant (<6/12) cataract and 70% of those over 85 years. Whilst age is the predominant risk factor for cataract formation, the process is multifactorial and remains to be fully elucidated. To date, surgery is the only effective treatment. Modern, small incision cataract extraction by phacoemulsification with foldable intraocular lens implantation allows rapid visual rehabilitation with low complication rates.
Indications for cataract surgery
■ Reduced visual function due to cataract.
■ Cataract limiting assessment or treatment of posterior segment disease.
■ Lens-induced disease (phacolysis, phacoanaphylaxis, phacomorphic angle closure).
■ Second eye cataract surgery to improve stereopsis and reduce anisometropia.
■ Refractive lens extraction (‘clear lens’ or ‘pre-cataract’), particularly in high ametropia.
History
■ Symptoms: ask about the duration and character of any visual loss (reduced VA, contrast sensitivity, or glare), and the impact on daily activities. Validated symptom questionnaires may help determine the need for surgery.
■ Past ocular history: spectacle or contact lens (CL) use, amblyopia, strabismus, previous anisometropia, glaucoma, surgery including refractive procedures, trauma, uveitis or
scleritis, and blepharospasm. In patients with a preexisting squint it is generally better to operate on the fixing eye first to avoid fixation switch and possible diplopia.
■ Past medical and surgical history: especially deafness, confusion, neck disease, orthopnoea, difficulty lying flat, and seizures.
■ Drug history: especially anticoagulants, tamsulosin (flomax), and allergies to iodine or antibiotics (some surgeons avoid subconjunctival cephalosporins in those with penicillin allergy due to the risk of cross-sensitivity).
■ Social history: identify pre- and postoperative social support and any occupational visual requirements.
Examination
■ Best corrected VA (BCVA): for near and distance and pinhole VA (PHVA, may indicate potential postoperative vision better than BCVA). Contrast sensitivity and glare disability are useful if symptoms are disproportionate to the VA loss, or the degree
of cataract.
■ Binocular balance: cover test and ocular motility.
■ Lids and adnexae: blepharitis, ectropion, entropion, orbital, or lacrimal disease may need treatment prior to cataract surgery.
■ RAPD: Check RAPD before dilating pupils.
■ Slit lamp examination: assess the anterior segment including corneal clarity, guttatae, anterior chamber (AC) depth, pupil size, evidence of previous intraocular inflammation or trauma, pseudoexfoliation, irido- or phakodonesis, IOP, and gonioscopy if angle disease is suspected.
■ Cataract: note the type (nuclear, cortical, posterior subcapsular, mixed) and grade (1+ to 5+) of cataract. Cortical cataracts are characterized by spokes, water clefts and
vacuoles due to osmotic imbalances in lens epithelial cells. Nuclear cataracts result from accumulation of protein aggregates in the center of the lens, becoming progressively
harder and more brunescent with time. Posterior sub-capsular cataracts occur at the posterior pole immediately beneath the lens capsule and are associated with the highest rates of cataract surgery.
■ Fundoscopy: note posterior vitreous detachment (reduced risk of postoperative retinal detachment) or vitreous pigment cells, and exclude optic nerve or macula disease, retinopathy and peripheral retinal breaks or degenerations (especially in high
myopes).
Investigations
■ Blood pressure: should be controlled preoperatively – there is an increased risk of suprachoroidal haemorrhage with systolic BP ≥180 mmHg or a diastolic >100 mmHg.
■ BM: diabetics may present with cataracts.
■ Other blood tests and ECG: only if clinically indicated – routine testing does not reduce morbidity and mortality. If taking warfarin ensure the INR is in the therapeutic range
(discontinuing warfarin increases the risk of stroke 1:100).
■ Special investigations: as indicated, including B-scan ultrasound to exclude retinal detachment or mass lesion if there is no fundal view; corneal topography (particularly if high or irregular astigmatism) to plan astigmatic surgery; specular microscopy and pachymetry to assess endothelial compromise.
Consent
■ Benefits: These may include
1. Improved quality of vision.
2. Improved fundal view to monitor or treat posterior segment disease.
3. Reduced spectacle dependence (a reading correction is usually required). More than 90% of patients (without coexisting ocular disease) achieve a BCVA of 6/12 or better.
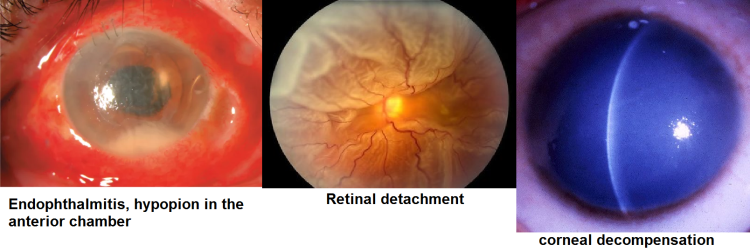
■ Risks: Complications are infrequent and most can be treated. The overall risk of blindness is 1 in 1000, with 1 : 10 000 chance of losing the eye as a result of surgery. There is almost no risk to the fellow eye. Potentially sight-threatening complications include: infectious endophthalmitis (0.1%), retinal detachment (<1%), suprachoroidal haemorrhage (0.1%), cystoid macular oedema (1–2%), and corneal decompensation (<0.3%). Other specific complications include: ecchymosis (common), posterior capsule rupture and/ or vitreous loss (<5%), dropped nucleus (<1%), postoperative IOP rise (common), subluxation of intraocular lens implant, iris prolapse/wound leak, uveitis, refractive surprise, spectacle correction for best vision, drop allergy, diplopia, ptosis, further surgery, and posterior capsule opacification. There may be a guarded prognosis if there is coexisting ocular disease. Patients with a longstanding unilateral cataract and a divergent eye are at risk of intractable postoperative diplopia.
■ Also discuss:
1. The diagnosis and natural history of cataract.
2. Alternative nonsurgical options such as spectacles.
3. The patient’s preferred refractive target and the risk of refractive surprise.
4. The surgical procedure, what to expect, and postoperative care.
5. Anaesthetic options: topical, LA or GA.
6. Admission: day case or inpatient.
7. Provide written information.
How to perform surgery:
